


Review Rating
5.0
Pre Surgical Infant Orthopedics
Nasoalveolar moulding (NAM) is a nonsurgical way to reshape the gums, lip and nostrils with a plastic plate before cleft lip and palate surgery.
Pre-surgery moulding may decrease the number of surgeries your child needs because it makes the cleft less severe.
The benefits of PNAM (Presurgical Nasoalveolar Moulding) are :
- Improved long term nasal esthetics.
- Reduced number of nasal surgical procedures.
- Effective retraction of the protruded premaxilla, and lengthening of the deficient columella, along with producing a limited maxillary growth disturbance in bilateral cleft cases.
Surgery is done after the moulding is complete, when your child is around age 3 to 6 months.
Read More

Treatment during Mixed Dentition
The treatment objectives for a child as he/she enters mixed dentition are directed toward preparing the patient for secondary alveolar bone graft (SABG) surgery. The alveolar bone graft surgery is typically performed around 9-12 years of age.
The growth of the craniofacial complex often accentuates a previously mild skeletal discrepancy. Patient evaluation includes an appraisal of the soft tissue condition (ie, presence or absence of oronasal communication); the skeletal aspects of malocclusion in all three planes of space; and dental problems, such as missing/malformed teeth, malpositioned/rotated incisors, anterior and/ or posterior crossbites. Discrepancies in maxillary arch form or transverse width should be improved before the SABG. Hence there is a need for alignment and expansion before the bone grafting surgery.
Cleft lip and palate patients often develop maxillary retrusion after cleft repair. The purpose of treatment in mixed dentition stage should be to achieve a favourable occlusion with positive overjet and overbite which can be achieved by means of anterior orthopaedic traction.
After SABG surgery, a postoperative CBCT must be obtained to confirm the outcome of SABG surgery. After successful repair of the cleft defect, the patient can then start Phase I fixed orthodontic appliance treatment is initiated to correct malpositioned anterior teeth and to help the graft stimulate by encouraging the eruption of the tooth in the question of the bone graft.
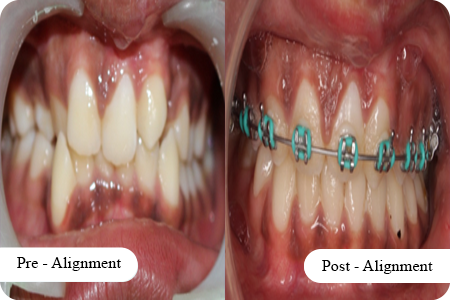
Read MoreTreatment during Permanent Dentition
Lateral cephalometric growth studies have shown that the maxilla in treated patients with cleft lip and palate show variable degrees of maxillary hypoplasia.The reasons for abnormal facial morphology in treated cleft patients may involve intrinsic skeletal and soft tissue deficiencies, iatrogenic factors introduced by treatment, or a combination of both.
Clinically, patients with clefts may present with a concave profile, midface deficiency, and a Class III skeletal pattern. The maxilla may also be deficient in transverse and vertical planes, contributing to posterior skeletal crossbite and reduced midface height. Dentally, there may be lingually inclined incisors and constricted maxillary posterior arch width, causing anterior or posterior crossbite. The extent of abnormal midface growth may vary from mild to severe. This requires orthodontic treatment for correction of malalignment before the orthognathic surgery.
Patients presenting with moderate to severe skeletal discrepancy may achieve the best aesthetic and functional results through a combination of orthodontic treatment that is carefully coordinated with orthognathic surgery. Depending on the severity of the skeletal discrepancy, the patient may require only maxillary advancement or a combination of maxillary advancement and mandibular setback. If the surgical/orthodontic option is elected, timing of the orthodontic and surgical treatment becomes critical.
Under optimal conditions, it is recommended to remove all dental compensations and to align the teeth in an optimal position relative to the skeletal base and alveolar processes. The orthodontist will plan the coordination of maxillary and mandibular arch widths by hand articulating the progressing dental study models into the predicted postsurgical occlusion. Once the presurgical orthodontic treatment goals are achieved (coordinated maxillomandibular arch width, compatibility of occlusal plans, satisfactory intercuspation), the patient may be debonded and placed on removable retainers until craniofacial skeletal growth is complete.
Read More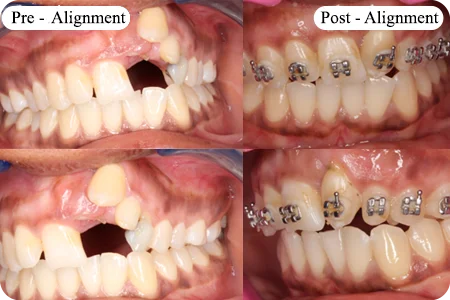
Our Doctors
Our Team
“THE PATIENT COMES FIRST" – is our team's motto and every member is committed to ensuring the complete well-being of our patients.










Advice and Resources
Advice and Resources
The journey of a child with cleft is long drawn and it is natural for parents or patients to have questions regarding the treatment or next stages.
We at Bhagwan Mahaveer Jain Hospital nurture and support an interactive holistic care where patients remain at the apex of our treatment goals, and we ensure they remain well informed throughout.
Please feel free to contact our team.